 Fuambai Sia Ahmadu, PhD Fuambai Sia Ahmadu, PhD This is an excellently produced anti-FGM video and the star, Kadija Gbla, is a powerful, passionate and dynamic speaker – I could use someone like her in my Crazy as We Want to be Campaign!! It has all the perfect ingredients of the western feminist anti-FGM horror story that the media has reproduced over and over again: First, the victimized African girl who comes to the West and receives enlightenment by White women about the oppressiveness of her own tradition; and second, that real female empowerment is acceptance of a universal truth… the clitoris rules!!! Hence, the triumph of western feminist clitorocentrism. Yes, what a suitable word - clitorocentric - that popped up from the protagonist herself (so no pun intended). Here’s the main problem with Khadija's uncritical acceptance of clitorocentrism and its supposed antithesis, so-called FGM: Like all other forms of discrimination politics – racism, homophobia and even sexism – clitorocentrism assumes the moral superiority of a dominant group (i.e. in previous times Caucasians, heterosexuals and men) over some perceived lacking, weakness or inherent evil of a minority group (usually physiologically based - such as race, sexuality and biological sex). In the case of clitorocentrism, it is clitorally “intact” women who are not just inherently sexually superior but more than that, they are “whole”, they are true women and they are thus, by definition, empowered. Those who have had their clitorises tampered with are defined, like other oppressed groups, by their perceived lack – in this case a whole, functioning clitoris. Suddenly, the biological essentializing that feminists at first rejected is now the hallmark (via the external clitoris) of the empowered modern, liberated woman. Where oh where is Germaine Greer...??? Clitoronormativity – Just like heteronormativity assumes the universality and naturalness of heterosexuality, clitornormativity assumes the universal appropriateness and naturalness of an “intact” clitoris. All other possibilities or ways of handling this part of the body is by definition wrong, unnatural, and just plain evil (because an intact clitoris is supposed to be the center and embodiment of female power). To be “clitless” is to be a victim and, as in many western countries, to be legally defined as a child. The western feminist led anti-FGM movement is not just about consent (in most countries, no adult woman can consent to female genital modifications – although this only applies to non-white women whose cultures do not uphold the sacred phallic value of an “intact” external clit). The moral tone and punitive intent of anti-FGM campaigns are about exercising power and forcing upon intransigent minority groups of circumcised women the views and preferences of the globally dominant group of clitorally “intact” women. Recruiting young women like Khadija to represent the supposed mutilation of all circumcised women is a way to reinforce clitoronormativity and silence the recalcitrant among us who reject a mutilated identity. Clitoromendacity – My word to describe the straight out misconceptions and deliberate propaganda about female circumcision that is fed to the media and regurgitated to the public. The most outrageous of these lies is that female circumcision practices completely remove the clitoris. There is no operation that can remove a girl or a woman’s entire clitoris and leave her alive. In Type I it is the clitoral hood or prepuce that is removed. In Type II what is excised is the clitoral glans and foreskin (see glans clitoris below). In Type III – the rarest form of female circumcision - the external clitoral hood and prepuce is sometimes excised or can be left “intact” and is stitched over with the labia majora. In all these types, the great bulk of the clitoral structure remains intact and very sensitive underneath the surface of the vulva. Many circumcised women (and western women who have had the external clitoral glans excised for health reasons) can achieve orgasm simply by manual or oral stimulation of the site of excision. The entire clitoris, as scientists are now discovering can be up to five inches in length and what is exposed is a small fraction – the tiny tip or head covered by foreskin. It is only in western feminist folk biology and popular culture that the external or visible glans and prepuce constitute the “entire” clitoris - biomedical science and African women from societies that practice female circumcision clearly know better. 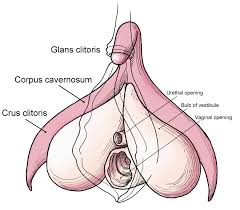 But what about the women like Khadija who are from these societies and have been traumatized by their experiences with lasting health and sexual dilemmas? And the thousands of women of all races, African women and African-American women who support the anti-FGM movement? Khadija links her brutal mutilation (at least how she claims to recall this) with all sorts of later gynecological ailments – heavy bleeding, fibroids and infertility. These conditions are pretty common among uncircumcised women and there are no studies that I am aware of that show a causal link of any these conditions with Type II excision that Khadija underwent. Notwithstanding, Khadija’s recollection of the horror she experienced in The Gambia, if true, is an example of what needs to change in the “underground” practices of female circumcision. It is possible that Khadija’s mother feared that once abroad, she would not be able to have her daughter circumcised and so she hurriedly recruited anyone who could perform a backdoor, crude procedure at minimal financial cost. It is important to note that what Khadija described is not typical of female circumcision in either Sierra Leone or The Gambia – except what we read about in western asylum cases. In these two countries that I am personally and professionally familiar with, female excisers are typically chosen for their experience, skill and reputation in performing traditional circumcisions and these operations customarily take place in large communal and ceremonial contexts. With respect to the main theme of Khadija’s message, her inability to experience pleasure – this is certainly also concerning. First of all, I think Khadija’s emphasis is actually on the experience of orgasm rather than sexual pleasure generally speaking. Again, here it is significant to note that there are many uncircumcised or clitorally “intact” women who do not experience orgasm. Study after study on female circumcision and sexuality have confirmed that the preponderance of circumcised women experience sexual pleasure and orgasm. And the fact that many circumcised women experience orgasm through manual or oral stimulation of the site of excision ought to suggest that excision per se is probably not the problem. In my view, when it comes to young women under the age of 40 who were born into or are living in western societies where circumcised women have been redefined as sexually mutilated, it is not surprising to find what one expert has referred to as “psychological infibulation” among female immigrants of this age group. In Dr. Lucrezia Catania’s sexuality study that compared two groups of women – a circumcised group of women from the horn of Africa that had undergone infibulation and a control group of “intact” Italian women - there were virtually no differences in women’s reported experiences of orgasms, sexual desire, frequency and so on (In fact the group of infibulated women actually reported slightly more frequent orgasms and more frequent sex with their partners).  What Dr. Catania’s team did observe was a generational difference in the reported experiences of the Somali group – younger girls who previously felt proud of their bodies and circumcisions in their home country then migrated with their families to western countries and came across the term FGM as well as countless images on the news, on youtube, basically all around them that told them they were victimized and mutilated. In Khadija’s case she recounted how at the tender age of 13 she started working for an anti-FGM campaign - albeit unintentionally at first. Khadija said she had blanked out her previous trauma at the age of six but then upon seeing the picture of Type II excision, everything came back and she could remember in vivid detail her horrid mutilation at the hands of her mother and some “old woman with a rusty knife”…where have I heard that before? Khadija attributed all her problems, heavy periods, painful sex, even fibroids and infertility to her FGM. She suddenly saw herself as "mutilated". She came to hate her mother and what she said her mother had done to her and had taken from her back in The Gambia. So, from the time she was a young teenager and presumably a virgin, Khadija bought into the idea that she would never experience pleasure and have an orgasm. Now, what I want to know is how any woman who has learned to hate her genitalia and to consider herself mutilated can truly relax and let go enough to bring herself or allow herself to be brought to the height of orgasm? It is not the presence of foreskin and a small mass of protruding tissue but a woman’s mind, her level of arousal, positive genital self-image and sexual confidence that enables her to break down her inhibitions and experience amazing bodily orgasms. And so it is thankfully that the vast majority of circumcised women in ethnic groups that uphold this practice do not see themselves as mutilated but as beautiful, empowered women and prefer the aesthetic effects of their modified genitalia. Most of these women in the major studies that have been conducted have very rich sexual lives, have orgasms and enjoy sex. In Sierra Leone, the very idea that women are not entitled to sexual pleasure is a ludicrous one and does not hold up with anyone who is familiar with the behavior and sexual confidence of circumcised Sierra Leonean women. As for my African and African-American sisters who are “uncircumcised” or clitorally “intact” or come from societies that do not uphold female circumcision practices, I can understand why many of them would side with the clitoronormativity of western patriarchal cultures. There is bodily identification and at least with some African and African-American women, a shared women’s movement and popular, globalized culture that has become very clitorocentric since the sexual revolution of the 60s and 70s. When the mainstream media makes itself available or accessible to the stories of the Khadija Glbas and not the views of the majority of women in our societies (who are stereotyped as stupid, backward and disempowered) then audiences only get to hear this terrible, greater than life horror story of FGM. When the only “facts” are those made available by anti-FGM activist organizations who work closely with WHO and UNICEF and other international organizations, then everybody is being misled. What is sad is the irony that although my African and African-American clitorally “intact” feminist sisters are ready to take sides and take up arms when it comes to denouncing FGM, they are silent about the increasing popularity of well-to-do, educated white women’s “female genital cosmetic surgeries” even on the genitals of underage white girls. As the western world enforces the global stigmatizing and criminalizing of even adult African women for exercising the same autonomy over their own bodies as our white female counterparts, I am left to ponder about what global sisterhood really means. Khadija is launching her own anti-FGM campaign in Australia because she says, with absolutely no evidence, that FGM is taking place rampantly in the country. Here in America, my Crazy as We Wanna Be campaign is requesting this evidence and more evidence to justify the persecution and prosecution of generally law-abiding if “clitless” African women immigrants in a dominant, clitorocentric and clitoronormative society.  Upcomiing blog Crazy As We Wanna Be explains the citorocentric meanings of female circumcision in West Africa... References
Ahmadu, F. (2007) “Ain’t I a woman too?”: Challenging myths of sexual dysfunction in circumcised women. In Y. Hernlund and B. Shell-Duncan (eds) Transcultural Bodies: Female Genital Cutting in Global Context. Rutgers University Press. Catania, L. et al (2007) Pleasure and orgasm in women with Female Genital Mutilation/Cutting (FGM/C) Journal of Sexual Medicine 4(2)1666-78. Public Policy Advisory Network on Female Genital Surgeries in Africa (PPAN). (2012) Seven things to know about female genital surgeries in Africa. The Hastings Center Report. Nov/Dec 2012.
6 Comments
|
Archives
March 2024
Categories
All
|
 RSS Feed
RSS Feed